SLAP Repair
Repair
SLAP Repair
Your shoulder comprises a ball-and-socket joint consisting of three bones:
- The upper arm bone, known as the humerus.
- The shoulder blade, called the scapula.
- The collarbone, also known as the clavicle.
The head of the upper arm bone fits into a rounded socket located in the shoulder blade, which is referred to as the glenoid. Encircling the outer edge of the glenoid is a sturdy, fibrous tissue called the labrum.
The labrum plays a crucial role in deepening the socket and providing stability to the shoulder joint. Additionally, it acts as an attachment point for numerous ligaments within the shoulder and one of the tendons originating from the biceps muscle in the arm.
SLAP Repair
The acronym SLAP stands for Superior Labrum Anterior and Posterior. In a SLAP injury, the upper (superior) portion of the labrum sustains damage. This particular area is where the biceps tendon connects to the labrum. A SLAP tear affects both the front (anterior) and back (posterior) of this attachment point. The biceps tendon may also be implicated in the injury.

Causes
Injuries to the superior labrum can stem from either sudden trauma or repetitive shoulder movements. An acute SLAP injury may occur due to:
- Motor vehicle accidents
- Falling onto an outstretched arm
- Forceful pulling on the arm, such as when attempting to catch a heavy object
- Swift or vigorous arm movements above shoulder level
- Shoulder dislocation
Individuals engaged in repetitive overhead sports, like throwing athletes or weightlifters, may develop labrum tears due to the continual stress on their shoulders.
However, many SLAP tears result from gradual wear and tear on the labrum over time. In individuals aged 30 to 40 and above, tearing or fraying of the superior labrum can be considered a normal part of the aging process, contrasting with acute injuries in younger individuals.
Symptoms
The typical signs of a SLAP tear resemble those of various other shoulder issues. They encompass:
Sensation of locking, popping, catching, or grinding.
Pain while moving the shoulder or maintaining specific shoulder positions.
Discomfort when lifting objects, particularly overhead.
Reduced shoulder strength.
Sensation that the shoulder might dislocate.
Limited range of motion.
Pitchers might experience a drop in throw velocity or a sensation of having a "dead arm" post-pitching.
Treatment
Non-Surgical
In many instances, the primary approach to treating a SLAP injury typically involves nonsurgical methods, such as nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen, which help alleviate pain and reduce swelling.
Another crucial component of treatment is physical therapy. Through targeted exercises, movement can be restored and the shoulder can be strengthened. These exercises focus on enhancing flexibility and range of motion, including stretching the shoulder capsule, which is the sturdy connective tissue of the joint. Strengthening exercises for the muscles supporting the shoulder not only alleviate pain but also help prevent future injuries. Typically, this exercise regimen lasts anywhere from 3 to 6 months and often involves collaboration with a qualified physical therapist.
Surgical
If your pain persists despite trying nonsurgical methods, your doctor might suggest surgery.
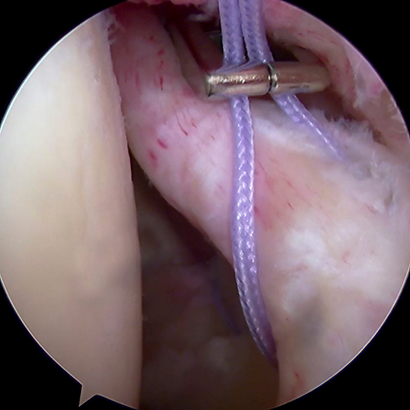
One common surgical approach for addressing a SLAP injury is arthroscopy. In this procedure, a small camera called an arthroscope is inserted into your shoulder joint by the surgeon. The camera displays images on a video monitor, guiding the surgeon's use of miniature surgical instruments.
Because the instruments and arthroscope are slender, the surgeon can make very small incisions instead of larger ones needed for traditional open surgery.
SLAP tears can vary in type, and the surgeon will decide on the most appropriate treatment once the injury is fully assessed during arthroscopic surgery. Treatment may involve simply removing the torn part of the labrum or reattaching it with sutures. In some cases, repairing with sutures may not be necessary, and instead, the biceps tendon attachment may be released to alleviate painful symptoms.