MPFL RECONSTRUCTION
Arthroscopy
Medial Patellofemoral Ligament (MPFL)
The medial patellofemoral ligament (MPFL) is an integral component of the intricate network of soft tissues responsible for stabilizing the knee joint. It connects the inner aspect of the kneecap (patella) to the long bone of the thigh, known as the femur. Together, the patella and femur form the patellofemoral joint. Injury to the MPFL typically occurs when the patella either dislocates or experiences partial dislocation (subluxation) due to trauma, often sustained during athletic activities or accidents. Certain individuals, particularly girls and women with naturally lax ligaments, may be more prone to such injuries, as well as those with unique variations in their bone structure. Individuals affected by these injuries are commonly diagnosed with patellar instability.

Injury to the MPFL
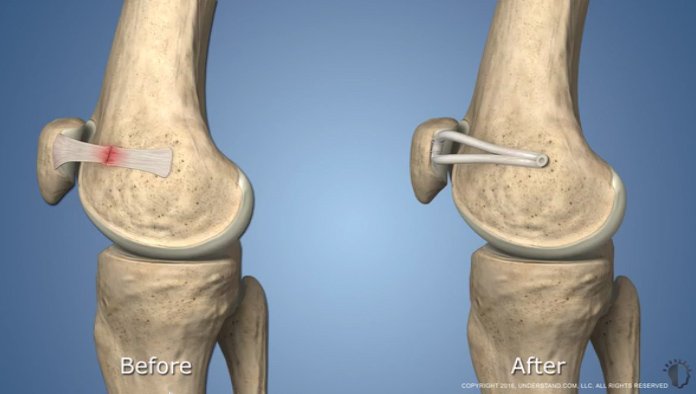
In a normally functioning knee, the bones within the patellofemoral joint move smoothly as the knee bends or straightens. The patella, or kneecap, smoothly glides within a groove in the femur bone. The medial patellofemoral ligament (MPFL) is crucial in ensuring the patella stays aligned within this groove, acting as a leash to control its movement. During a patellar dislocation, the soft tissues endure damage as the patella dislodges from its groove and then forcefully returns to its place. Because the dislocation typically happens towards the outer side of the leg, the MPFL ligament inside the knee often tears. If left untreated, a torn MPFL can heal naturally but often in a weakened and lengthened state. This can lead to instability, increasing the likelihood of future dislocations and potential damage to the knee's cartilage. While the immediate pain, swelling, and impairment from a dislocated kneecap are concerning, the greater risk lies in subsequent damage to the cartilage. Once this cartilage deteriorates, the risk of developing patellofemoral arthritis significantly increases, posing a more challenging condition to manage. Given these risks, it's always advisable to seek treatment aimed at preventing further kneecap dislocations.
MPFL Reconstruction
MPFL reconstruction surgery involves the creation of a new medial patellofemoral ligament to stabilize the knee and prevent further joint damage. This procedure provides a promising treatment for individuals who have undergone multiple dislocations. While historically, patients with MPFL damage had limited treatment options such as immobilization and rehabilitation, surgical tightening of the damaged ligament showed some benefit. However, MPFL reconstruction is a relatively new procedure, with its efficacy becoming more recognized in recent years, particularly since around 2006.
Post-surgery
What to expect after MPFL Reconstruction
Following MPFL reconstruction, patients are permitted to bear weight on the affected leg, which is then secured in a brace for a duration of six weeks. The brace serves to maintain the leg in a straight position during walking. As part of the recovery process, a Continuous Passive Motion (CPM) machine is employed at home to prevent the formation of scar tissue and stiffness in the joint during the healing of the ligament. The CPM machine facilitates movement of the patellofemoral joint without requiring the patient's muscular effort. Upon achieving sufficient strength in the quadriceps (the major muscle in the thigh) to support the joint, patients can initiate physical therapy, typically around six weeks post-surgery. Additional methods to expedite recovery include utilizing devices that administer electrical stimulation to the muscles surrounding the knee, as well as the utilization of Game Ready, a machine designed to compress and cool the leg, thereby diminishing swelling and discomfort. It should be noted that the cost of these devices may not be covered by insurance. In general, individuals can anticipate a return to sports or other physical activities within a timeframe ranging from 4 to 7 months following MPFL reconstruction. However, it's important to recognize that recovery periods may vary and are contingent upon factors such as individual anatomy, healing capacity, and pre-surgical health status for those considering this procedure.